
A patient presented following a fall resulting in severe trauma to the four maxillary incisors. Clinical
examination showed extensive structural damage affecting the upper central and lateral incisors, with the
teeth considered unrestorable. The case required management of both the immediate consequences of
trauma and the long-term restorative challenge in the anterior maxilla.
Clinical Assessment
The patient’s main concerns were pain, appearance, and the loss of function in the upper anterior region.
Clinical assessment identified significant fracture and compromise of the four upper incisors. In addition to the
dental injury, attention was given to the condition of the surrounding soft tissues and the aesthetic implications
of treatment in the smile zone.
Pre-operative clinical views demonstrated the extent of the trauma and the compromised condition of the
maxillary incisors . Radiographic assessment was carried out to evaluate the remaining bone support and to
guide implant planning. The aim was to provide a fixed restoration with good functional and aesthetic
predictability while minimising surgical intervention.
Treatment Planning
As the four maxillary incisors were unrestorable, extraction was indicated. The restorative plan was to replace
the missing teeth with a four-unit implant-supported bridge retained on two implants.
This treatment approach was selected to:
Restore function and aesthetics in the anterior maxilla
Provide a fixed long-term solution
Optimise implant distribution within the available bone
Avoid unnecessary placement of additional implants where not required
In anterior cases of this type, implant positioning is critical not only for support of the prosthesis but also for
emergence profile, soft tissue contour, and overall smile aesthetics.
Surgical Phase
The four upper incisors were removed with care to preserve the surrounding tissues as much as possible.
Following extraction, two implants were placed in strategic positions to support the planned four-unit
bridge.
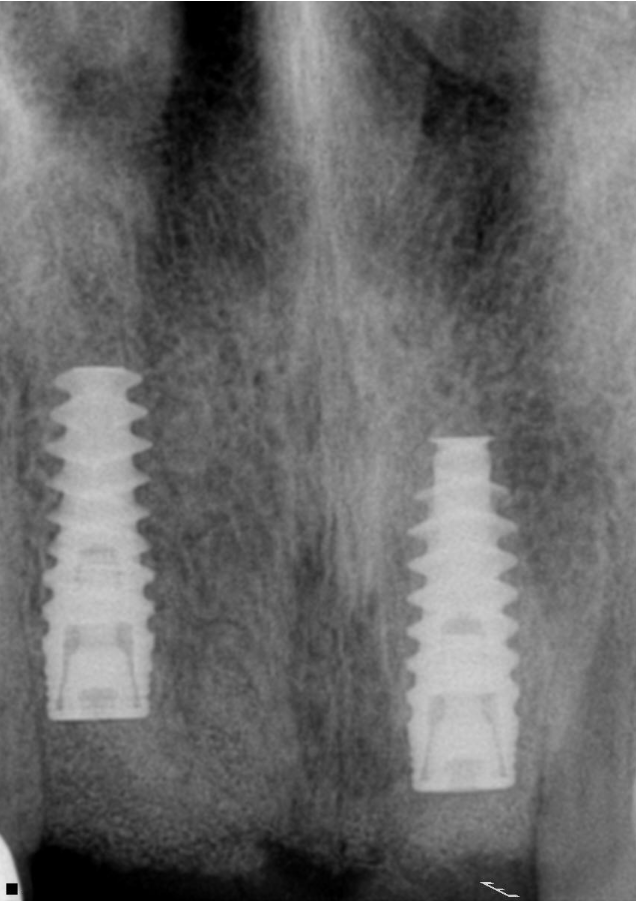
Achieving appropriate three-dimensional implant placement was essential. Particular attention was paid to
angulation, spacing, and restorative-driven positioning in order to support an acceptable prosthetic
outcome. Primary stability was achieved at placement, synthetic bone grafting was utilised to fill the space
around the implants, and postoperative radiographic review confirmed satisfactory implant positioning.
Osseointegration and Prosthetic Phase
A healing period was allowed for osseointegration before proceeding to the definitive restoration. During
this period, the patient was monitored clinically to assess tissue maturation and implant stability.
Once integration had been confirmed, the implants were restored with a four-unit bridge replacing the four
maxillary incisors. The prosthesis was designed to provide:
Adequate anterior aesthetics
Functional incisal support
Acceptable phonetics
Cleansability and long-term maintainability
The final restoration re-established continuity of the anterior dentition and provided the patient with a fixed
replacement following traumatic tooth loss.

Discussion
Trauma affecting multiple maxillary incisors presents both surgical and restorative challenges, particularly
in the aesthetic zone. In this case, replacement of four incisors using two implants and a four-unit bridge
offered a conservative and effective fixed solution.
Success in such cases depends on careful diagnosis, prosthetically driven implant placement,
preservation of hard and soft tissues, and close attention to the restorative design. Where these principles
are followed, implant-supported bridgework can provide predictable functional and aesthetic rehabilitation
after traumatic tooth loss.
Conclusion
This case illustrates the management of severe trauma to four upper incisors using extraction, placement
of two implants, and restoration with a four-unit implant-supported bridge. The treatment provided a
stable, aesthetic, and functional outcome, demonstrating a practical approach to rehabilitation in the
anterior maxilla following trauma.